SHOULDER PAIN · DECISION GUIDE · LOGANSPORT, IN
Rotator Cuff vs. Impingement vs. Frozen Shoulder: How to Tell (and What to Do First)
They’re commonly confused — but the best first step differs.
If you’ve been told “it’s probably your rotator cuff,” you’re not alone. Use these pattern checks to narrow what’s most likely, then pick the safest first step. For the broader overview, see Shoulder Pain: 7 Common Causes and the care page Shoulder Pain Treatment.
- Quick answer + table + first-step plan
- Designed for lifters, workers, and busy humans
- Clear “when to worry” red flags included below
Educational only. Not medical advice. Seek urgent care for severe/worsening symptoms or red flags.
Quick Answer (If You Only Read One Section)
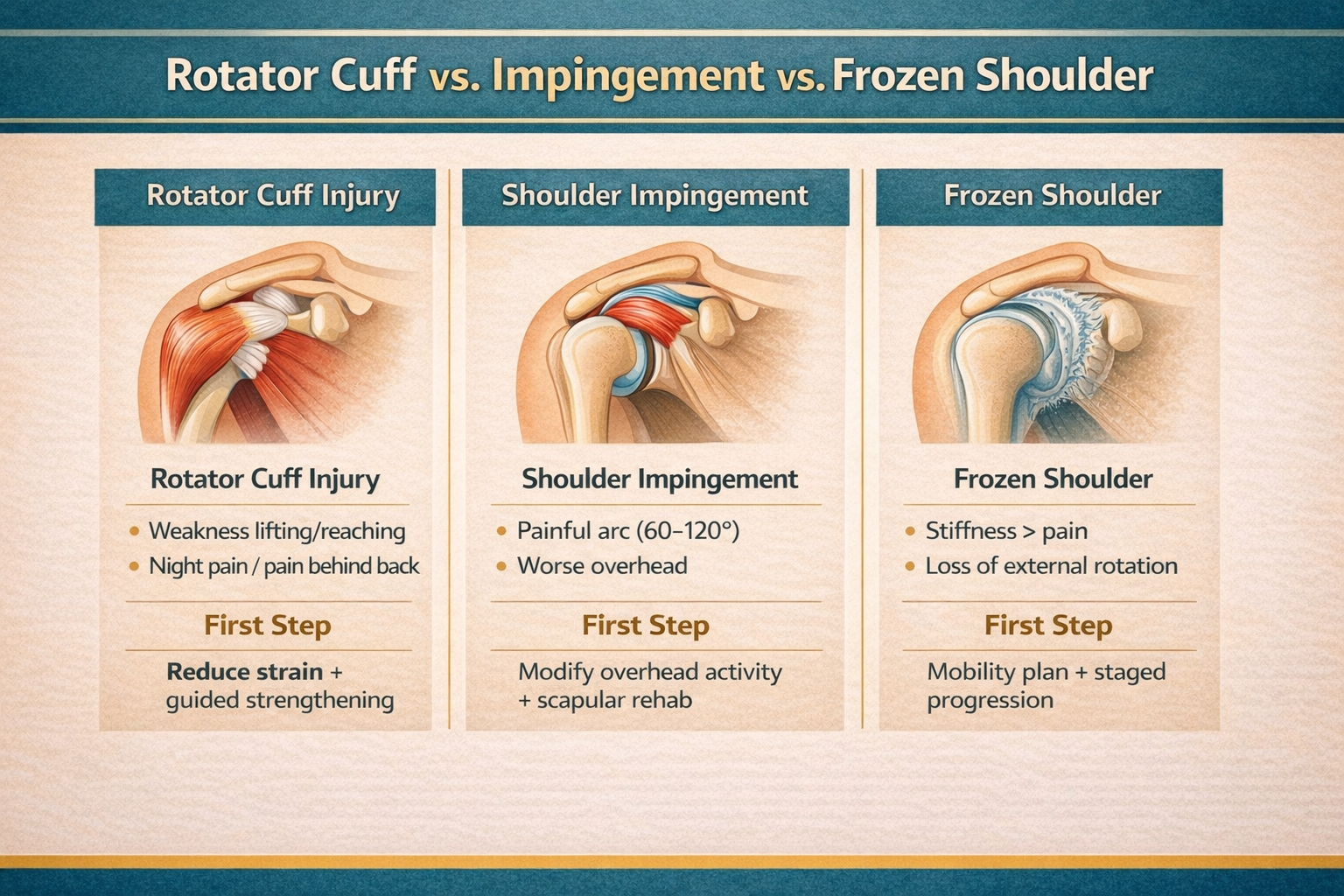
Frozen shoulder is dominated by stiffness and a “blocked” feeling. Impingement-type pain often has a painful arc with overhead activity. Rotator cuff irritation behaves like tendon overload—pain with lifting/lowering and common night pain.
Best first step (simple rule)
If range of motion is progressively disappearing, treat it like a stiffness pathway. If motion is mostly there but overhead is cranky, treat it like mechanics + load. If lifting/lowering is painful (and night pain is common), treat it like tendon overload.
Comparison Table (Fast, Skimmable)
This isn’t a diagnosis — it’s a way to choose the right direction and avoid the wrong plan.
| Feature | Frozen Shoulder | Impingement-Type Pain | Rotator Cuff Irritation |
|---|---|---|---|
| Dominant feel | Stiff + blocked | Pinch/painful arc overhead | Tendon overload (lift/lower pain) |
| Range of motion | True loss (esp. external rotation; behind-back) | Often available but painful in certain angles | Often mostly available; strength tests can hurt |
| Classic trigger | Reaching behind back; rotating outward | Repetitive overhead work; certain angles | Lifting away from body; lowering from overhead |
| Night pain | Common | Can happen | Common |
| Best first step | Staged mobility + irritation management | Scapula mechanics + mobility + graded strength | Load management + tendon-focused strengthening |
| What NOT to do | Force sharp stretches | Keep testing painful overhead reps daily | Keep pressing through pain without modifying load |
Quick Pattern Checks
Use these to narrow the bucket — then confirm with an exam if symptoms persist.
Frozen Shoulder (stiff + blocked)
Key sign: you feel “stuck,” especially rotating outward and reaching behind your back.
First step: consistent, low-intensity mobility (not aggressive forcing) + a staged plan.
Impingement-Type (painful arc)
Key sign: pain through a slice of the lift (often 60–120°), worse with repeated overhead work.
First step: scapular mechanics + thoracic mobility + gradual strengthening.
Rotator Cuff Irritation (tendon overload)
Key sign: pain/weakness with lifting away from the body and lowering the arm; night pain is common.
First step: load management + tendon-strength progression + technique cleanup.
Not sure? Here’s the safest default
Stop repeatedly forcing painful overhead reps for a week, keep pain-safe motion daily, and choose a plan matched to your best-fit bucket. If you’re losing motion week-to-week, treat it as a stiffness pathway and get evaluated.
What to Do First (Action Ladder)
Simple steps you can follow without guessing.
First 72 hours
- Reduce the one movement that reliably spikes pain (usually overhead / deep pressing)
- Keep pain-safe motion (don’t immobilize)
- Stop “testing” the painful angle multiple times per day
Next 7–14 days
- If you suspect rotator cuff overload: bias pulling/upper back work and build pain-safe strength
- If you suspect impingement-type: add thoracic mobility + scapular control and adjust pressing angles
- If you suspect frozen shoulder: daily staged mobility without forcing sharp pain
Weeks 2–6
- Progress range first, then strength
- Reintroduce overhead gradually only when tolerance improves
- For lifting-related issues, read: Lifting Shoulder Pain Fixes
When imaging is more reasonable
- Significant trauma + major weakness, deformity, or severe swelling/bruising
- Progressive loss of motion week-to-week
- Stalled progress despite a smart plan and good adherence
When to Worry (Red Flags)
Get urgent evaluation if any of these are present.
- Deformity after injury, suspected dislocation/fracture
- Inability to lift the arm or sudden major weakness after a pop/injury
- Sudden severe swelling/bruising
- Fever with a hot/red shoulder
- Chest pain/shortness of breath or concerning systemic symptoms
- New numbness/weakness down the arm
If you’re unsure, start with Contact & Location and we’ll guide you.
Rotator Cuff vs. Impingement vs. Frozen Shoulder FAQs
Quick answers—including “when to worry.”
Leave a Reply